We just came back from our annual Spring visit to see our grandson in Ohio. Some thoughts on what’s changed, what hasn’t, or just what I noticed, in no particular order.
Covid is done. Over. No mas as we say. Yes, it is still circulating, and there will be more variants, and some people will need more boosters, and others will get sick and may even die. But the heavy weight that was the pandemic is lifting. We didn’t see a mask after we left the airport. They are not required in Ohio; although businesses may require them, they don’t. Covid is becoming an endemic disease not as defined by the medical community, but in the res publica, the community. People have decided to move on. It would take something truly shocking to change that direction, and a CDC announcement won’t do it.
People are a little friendlier. With masks gone, and with limited human contact for so long, people seem just a little more open to a “good-day” or a “hello.” I’m not talking a habitual “buenos dias” here, but still, it’s noticeably friendlier. However . . .
There are still many people on the edge of losing it. As in becoming violent for little or no reason. I did not see such things, but the news and social media are full of stories. Road rage, kids bringing guns to school, attacks on flight attendants, hey even let’s slap-the-crap-out-of-Chris Rock on national television. It may be years before all this suppressed anger works its way out of the body civil and politic.
Inflation is real, it is increasing, it is a problem, everyone is talking about it, and the administration has no idea what to do about it. On past visits, everybody was talking about Covid; now it’s prices. And all the government and political talking heads are saying is gibberish about who is to blame. It bears repeating that government at all levels has difficulty dealing with inflation, but it’s not like the US (and other countries) have never experienced it before. It won’t get better for a long time, because nothing is being done.
I know change is a constant, but sometimes it hits you when you least expect it. We flew to Chicago (tip for lakeside expats: Delta/AeroMexico have non-stops to/from O’Hare!) and drove to Cincinnati. As we left the Chicago suburbs in neighboring Indiana, I told my dear wife we would be driving on I-65, a rural interstate highway to Indianapolis, so traffic would be much better. I knew this because I went to high school in the area, and even took part of my driver’s test on that interstate. But that was forty-six years ago and I had no idea how far the sprawl had spread, and how much traffic there was now on that road. And we passed through an immense Windmill farm, too. I’m talking hundreds of the giant creatures, silently spinning over the corn-and-soy fields of Indy. Wow. Meadow Lake windmill farm, over 400 turbines!
And still growing!
Speaking of green energy and climate change, I have this story to relate. As we walked and talked about the suddenly cold weather one day, my fifth-grade grandson blurted out, “we’re doing such a terrible job with the environment, the world’s going to end in ten years.” Now, he’s a bright kid, and what he said bore no trace of hyperbole, sarcasm, or irony. He doesn’t watch any TV (except sports) and has limited screen time, which he mostly uses on games or programming (no social media). So I asked him where he heard that; he explained they “spent a bunch of time on it in school.” Just a fact, as he had been taught. Whatever your feelings about climate change, the notion all we have is ten years is a ridiculous assertion, and certainly not appropriate for middle-schoolers. It’s an exaggeration based on the Intergovernmental Panel on Climate Change (IPCC) report stating we have ten years before we hit another (bad) milestone in the warming of the planet. And we wonder why childhood depression and suicide rates are rising.
Political advertising seems to keep finding new lows. There are party primaries approaching in Ohio, and the attack ads are flying full of vitriol. “Liar” is a common descriptor, and I believe I heard at least one “coward.” “Shameful” was frequently invoked, and I agreed, much of the work was shameful.
Traffic at airports and on planes has almost recovered. We saw few empty seats and long lines at the airport concessions. We also saw a lot of infrastructure work going on, perhaps related to the bipartisan infrastructure bill passed by Congress and signed by President Biden. Long overdue, and welcome even if it causes some congestion and delays.
Glad to be back from the variable highs and lows of Cincinnati to the sunshine and steady warmth of Ajijic. Here’s hoping that the mask mandate is gone before our next trip in May!
Another partisan issue is voting; Captain Obvious would agree. After all, voting involves choices among parties (in most places), so who gets to vote and under what circumstances is obviously a matter up for partisan debate. Some democracy advocates would disagree saying “it’s a fundamental human right” and the UN Declaration on Human Rights supports this view. Yet even fundamental rights have limits: children don’t vote, and no one seems to get upset about that.
In the United States, there are two camps–both extreme–currently waging war over voting rights and procedures. On the right, Trump supporters claim the 2020 election was rigged, full of vote fraud which illegally denied then-President Trump a second term. In his supporters’ view, this fraud requires a tightening of voting rules and greater oversight by State elections officials, up to and including the ability to overrule and replace slates of electors in future elections. On the left, the push to enact greater restrictions is seen as an attempt to disenfranchise (mostly) minority voters who vote overwhelmingly for Democratic Party candidates, and to build in an illegal backstop to overrule majorities and ensure Republican electors in the future. Their meme is “Jim Crow 2.0” recalling the many ways southern states denied black Americans their franchise for almost one-hundred years.
As I usually admit, both sides have basic facts to support their contentions, but both exaggerate or outright lie to make a stronger case. Let’s examine the whole truths, shall we?
For starters, the notion everybody has a right to vote. Advocates chant this, but no one, and I mean NO ONE, really believes it. Children (as noted) don’t deserve a vote. People who are unconscious don’t merit a vote. You and I may disagree about how young is too young, or how conscious someone needs to be, or if felons or non-citizens should be allowed to vote. But the principle stands: some people do not have a right to vote. In fact, the original text of the US Constitution said very little about who could vote, other than that if one was eligible to vote in one’s state, one was eligible to vote for federal office. States were left to decide the franchise, that is, who could vote.
Much is made of the sexism and racism of the original state decisions to limit voting to white men who owned property. This was more a case of elitism than anything else (since it disenfranchised more white men than women or blacks). It was elitism to believe (as those passing the laws feared) that large groups of voters could be bought or directed by others. Yet even the white men of property all knew of cases of ‘saloon meetings on election day’ when wealthy candidates bought rounds of drinks for eligible voters in exchange for trips to the voting booths. More voters simply meant more opportunities for fraud in this view.
Drunk & ready to vote!
And the history of American politics is rife with voting fraud. Anyone familiar with the two centuries of Tammany Hall control of New York City or the Daley machine’s sixty-year run in Chicago knows that such organizations knew precisely how much corruption and vote fraud was needed for every election, from ward member to President. Top those stories off with the hundred years of poll taxes, rigged literacy tests, and violent intimidation of black voters under Jim Crow laws. It was very late in the Twentieth Century that most of the blatant voter fraud and disenfranchisement was wrung out of the US democratic process, at the cost of many new laws and controls.
But’s that all (dirty) water under the bridge: what about today? One cannot see today’s exaggerations for what they are if you don’t know the history!
Let’s start with the fraud claims in the 2020 election. President Trump and lawyers representing him filed sixty-three lawsuits claiming voter fraud. They were heard in a variety of states, under various Republican- (including Trump) and Democratic-appointed judges. All of these suits were denied, most in summary judgments. That is, the attorneys filing the suit made claims, but when asked by the judge to present ANY evidence to support the claimed fraud, they did not do so. So it’s not a matter of not considering the evidence; no evidence was produced. Some lawsuits presented evidence, but never in sufficient numbers to affect the outcome of the election in that state, rendering the suit moot. Some more outrageous claims, like those of rigged voting machines, are not being adjudicated as (disproven) vote fraud accusations but as defamation by the individuals making the claims. Even various recount efforts by pro-Trump organizations and legislatures have failed to find anything which undermines the legitimacy of Biden’s 2020 victory.
Why do so many Trump supporters (and even Republicans in general) still believe the election was rigged after this unbroken record of failure? First off, there is the recent historical precedent. What’s good for the (Democratic) goose is good for the (Republican) gander. Democrats clung to the 2016-election-was-rigged-and-Trump-is-a-Russian-stooge fairy tale to this day, and Trumpers love a good tit-for-tat. Second and more importantly, the 2020 election was held during a pandemic which made for really dicey voting conditions and delayed outcomes. States changed voting rules and procedures, often late in the election cycle, in a genuine attempt to assist voting when gathering in public on election day may not be advised or even permitted. Some of these changes violated State constitutions and were thrown out; most were allowed as prudent responses to an unprecedented situation. In general, these rules favored absentee/early voting.
Nothing wrong with absentee/early voting, although it does require special and different forms of verification than in-person voting. States like Colorado had pioneered the effort and had strong procedures in place. But other states tried to enact new early/absentee processes on the fly, while the government officials responsible for implementation were not even working in-person. This led to debates about fairness, ballot verification, voter identification, drop-boxes, and nursing home ballot harvesting. None of these situations demonstrated any fraud which could have changed the state’s electoral outcome. But they did delay vote total announcements, and that was a major problem.
As predicted by several analysts, the delayed announcements of voting results were inevitable, and had an obvious effect: Republicans tended to favor in-person voting, where rapid processes were in-place that resulted in quick vote totals. Democrats favored absentee or early balloting (the kind that took longer to count). This resulted in election night preliminary results indicating President Trump would be re-elected, and morning-after results showing he lost. Which the President and his supporters were never going to believe, no matter how many recounts, lawsuits or fact checks were done. Hey, some on the left still believe that Al Gore beat George W. Bush, so delusion is bipartisan.
Now some red states are rolling back the pro- early/absentee processes they enacted during the pandemic, and some Democrats are crying foul. The amusing thing here is (1) there is no evidence the changes increased the number of Democratic votes, and (2) there is no evidence the changes increased the total number of votes. The 2020 election was a vast experiment with red and blue states making different choices about voting rules, but with an odd outcome: the changes neither affected the total turnout nor the partisan results. And this tracks with decades of research on the issue. So Republicans are doing something meaningless in terms affecting Democratic voters, and Democrats are fighting it even though it doesn’t make a real difference. This may be the ultimate “no there, there” issue. What did happen is when people voted changed (Democrats early and absentee, Republicans in person on election day), but not the number of people voting. Furthermore, some of the red state changes are the same as or less restrictive than those which already exist in blue states, which hardly is evidence for claims of “Jim Crow 2.0”. Georgia has been the principle battleground for these charges. If you want a solid review of what’s changing and why, Georgia Public Broadcasting has it here. Suffice it to say the changes place Georgia in line with voting processes in New York, and New Jersey, and even Delaware, so Jim Crow is more widespread than we knew.
Gerrymandering remains a problem, but I note that the same folks who decried it as a great Republican threat to American democracy (sic) are now chuckling at the Democratic party’s clever use of it to secure more seats before the 2022 mid-terms. Perhaps it isn’t quite the existential threat some imagined.
States may find a way to limit gerrymandering, but I am not optimistic. It must be done using State constitutions, not the federal one, since the US Supreme Court has called gerrymandering an unfortunate but inevitable fact of electoral life (my words). The move to create new or additional review mechanisms to certify an election is troubling, and might provoke a constitutional challenge if implemented. Oddly enough, some state legislatures once appointed their own choice of federal electors, regardless of the votes cast, in effect treating the vote as a popularity contest. However, once a state commits to using an election to determine slates of Presidential electors, it would be legally dubious to somehow ignore the results and select other electors. And the US House of Representatives need not accept them (another thing which already happened).
Finally, there are those who claim that since there is no widespread evidence of voting fraud, there is no reason for new or additional restrictions on voting. Those holding this view are guilty of the magic amulet fallacy (“See this magic amulet; it keeps away tigers.” “I don’t believe it.” “You don’t see any tigers, do you? It must be working!”). Voter fraud has always been an issue, and it was one mitigated by increasing identification and verification processes. If the states wish to move toward more options for voting (early, absentee, online, whatever) they need to enact more and better processes to prevent voting fraud, which will occur. One need not be an alarmist or a racist or a partisan, just familiar with history and technology, to see why.
In summary, Republicans are attempting to suppress Democratic votes, and vice versa. The fact that one side seems more successful (in passing new rules) is not a moral judgment. More importantly, there is no evidence the changes make the difference that is (privately) believed by the Republicans or publicly-decried by the Democrats! That fifty-state experiment in 2020 showed that the increases in voting, and the partisan shifts, were the same in blue and red states and in states with fewer/more restrictions. The 2020 federal election was legitimate, as was the 2016 one. All that changed is when people voted: Democrats before the election, Republicans on election day.
Most importantly, don’t question the legitimacy of the election process, and remember to vote!
Ever wonder why the prices at gas stations go up so fast, but come down so slow? Not around here, where PEMEX continues to own most stations and even those run (under an aborted attempt to introduce competition) by other oil giants must buy their gas from PEMEX! But it’s a common enough phenomenon in the States as to anger the average person.
Ask your favorite liberal/progressive, and it’s a conspiracy of sorts. President Biden and some of his spokespeople coined #PutinPriceHike to blame the rise on everybody’s least favorite authoritarian. Putin certainly isn’t helping, but gas started rising long before the war in Ukraine. Senator Elizabeth Warren beat a familiar war-drum: “The cause of rapidly rising energy prices for consumers and manufacturers is clear: some of the nation’s largest and most profitable oil and gas companies are putting their massive profits, share prices and dividends for investors, and millions of dollars in CEO pay and bonuses ahead of the needs of American consumers and the nation’s recovery from the pandemic.” Big Oil profits are at or near record levels. From the conservative side, pundits blame Joe Biden for cancelling the Keystone pipeline and pausing new drilling leases on federal land. Yet a pipeline doesn’t increase production, and thousands of leases remain unused. What’s really going on here?
Strap in, this may take a while, and if you’re open-minded and not careful, you might learn something!
Is Fat Albert cancelled?
All these claims have some truth: the best propaganda always does! But none of them captures the whole story, which is far more complicated (bad) but also interesting (good). I’ll attempt to make it simple:
After in-depth research, I uncovered this unassailable fact: not a single one of the major oil companies (hereafter Big Oil)– neither ExxonMobil, nor bp, not Chevron or Marathon–is registered as a 501.c.3 charity; look it up. Apparently, all of them are for-profit enterprises; I know you’re shocked. And as such, they try to make more (and more, and more) profit, all the time. There is a technical term for businesses which don’t seem dedicated to profiting: bankrupt. Not that this justifies just any old behavior (like price-fixing or profiteering, just to name two), mind you, but also keep in mind that there is an entire part of the federal bureaucracy (in the Justice Department) which spends all its time looking for such things. So don’t be surprised when Big Oil makes money, and know that someone is always looking over their shoulder if they do it the wrong way.
Let’s look at the other end of the spectrum: the price at your local pump. It is there the pain is felt, and no, you’re not imagining it: prices do go up faster than they come down. Is that Big Oil? Big Oil owns around one percent of the gas stations in the US; the rest are independent or have affiliations, which are unique supply contracts (if you’re a bp station, you only offer bp gas and products). About fifteen cents of the cost of each gallon of gas goes into paying for the overhead of owning/running a station: breaking even for the gas station owner means charging 15¢ over the price he/she paid. Most look to charge about two cents more for profit (yes, gas stations on average make just two cents profit per gallon). The federal and state governments also tax gas sales: so different tax rates in different states are another cause of price differences.
Gas stations fill their tanks between once and twice a week, and the price they pay changes constantly. So they are in a slim margin business with high volatility; the only saving grace is most everybody needs their product, and people like to re-use the same stations for convenience. But the gas station owner might be selling gas he bought last week for a price he is anticipating next week (cheaper or dearer). Guess wrong one week, no problem. Guess wrong too many weeks: bye-bye. So they generally raise prices faster and lower them slower. Note, we’re not talking about huge profits here. Why not? Because the gas station across the street gets its gas deliveries on different days, and is facing the same challenge. If the first station raises its prices too soon or too much, the second station gets more business. If it happens all the time, the first goes out-of-business. Ahhh, competition. I’m sure we all have stories of gas-price wars which resulted in some amazing deals-at-the-pump.
Standardized price of oil (blue) and retail gas (green) over decades
And in case you were wondering what the biggest cause of retail gas prices is, the chart above shows the correlation between oil prices and retail gas prices. This is what we call a strong correlation, almost certainly causation. There are only minor times–usually a result of some crisis or shock to the global supply chain, where the two prices don’t vary directly. But what about Big Oil’s massive profits? Don’t they prove price gouging?
I’m am sure you heard that ExxonMobil raked in $23 billion in profit in 2021. The same goes for all Big Oil. But did you know ExxonMobil lost $22.4 billion in 2020? Their net profit for two years was $600 million, which is nothing compared to revenues. All Big Oil took a huge hit in 2020. They went on a down-sizing binge (cutting costs) and started selling off assets that didn’t fit with (some of) their commitments to move away from fossil fuels. The combination of a large drop in expenditures, profits from businesses they sold, and the rise in oil prices resulted in . . . record profits. Not gouging, not conspiracy, just a fortunate turn after a very, very bad year. Apple is the world’s most profitable company, with 2021 profits of almost $153 billion, also a record year; where’s the concern for that number, which came after two previous record years of profit?
Big Oil is a very robust industry, for a reason. They pioneered the concept of scenario planning. With the long-lead times for production, market volatility, and vulnerability to geopolitics, they had to! Royal Dutch Shell–as it was then named–pioneered the process of looking at alternative futures way back in the 1970’s, and used the work to anticipate things like the 70’s oil shocks and survive them as a business. I attended an executive education seminar at Oxford in the early 2000’s, and we were still studying Shell’s techniques then!
Speaking of long lead times, what’s up with all those leases President Biden mentioned? And what happened to the US fracking revolution, which made us energy self-sufficient during the last administration? It can take decades to go from field exploration to buying leases to approving permits to putting in the drill rigs and pipelines to pumping oil. These are costly endeavors which may or may not produce marketable oil. Companies speculate on leases, buying some on the prospect there is oil and others to keep them out of another company’s hands. After you acquire a lease (for example, from the US federal government which owns about about 47% of all land out west), you still have to do research on the site, and test for suitability of the site and the oil. If it passes, you must begin the permitting process, which involves sate regulators and environmental agencies and activists. All this process is proper, but imagine how long the studies and lawsuits take. Then comes erecting the drill site and laying the pipeline, and finally, pumping oil. The outlays prior to any possible revenue are huge, and must be accounted for by the revenues resulting from the drilling which does produce. There is nothing unusual or sinister in the number of non-drilled leases held by Big Oil right now. Those decrying the President’s moratorium on federal leases are also just making noise. And all those saying these things know better.
The fracking revolution did itself in. Hundreds of small US companies used the fracking technique to generate sizable increases in US oil production, making the US the world’s largest producer at one point. The competition between the frackers was cut-throat, and OPEC dearly wanted to starve them out by increasing production of Saudi (and Russian) oil at less cost. Then came the Covid economic collapse, which Big Oil survived, but which doomed many frackers. The remaining fracking companies are being more careful about capital investments and profitability, acting more like Big Oil and less like internet start-ups.
Likewise, new pipelines do not increase production. If there is excess production somewhere in the system, and excess refining capacity somewhere else in the system, a pipeline between the two locations can increase overall production, but only in this relatively unusual case. Most pipelines are simply more efficient means of transport, which is not a bad thing, but hardly a near-term solution to anything. Oh, and pipelines face all the same regulatory hurdles as the drilling sites, so no, they are not fast.
Which brings us to “the Turn.” The Turn is the common term used by green energy advocates AND Big Oil for the move away from fossil fuels. British Petroleum even legally changed its company name to “bp” and started citing themselves as “beyond petroleum” (no, no one believed it). Big Oil and green energy advocates use the same phrase, but mean very different things, and the concept has implications for today’s gas prices. As in, if oil prices are high and Big Oil profits are up, and they want to make more profit, why don’t they starting producing more oil? I have explained how it takes time, but Big Oil is not even doing those smaller, simpler things they could to increase oil production immediately. What gives?
What is the future of the energy business?
Not a quip; he said it over and over
If you ask any environmental group, anyone concerned about climate change, anybody in the automotive or energy business, they will agree. The Western model of economic development based on the Petroleum, Oil, and Lubricants (hence POL) used by the Internal Combustion Engine (ICE) has been wildly successful, but must come to an end. It was labelled the POL-ICE connection and it is an ongoing revolution in the developing world. Those most concerned about climate catastrophe say it must end now or soon, like in ten years. The industrial giants (including Big Oil) think thirty-forty years, with some residual use after that. But it will end, and it must be replaced with some other energy source.
A gallon of gas was about the same $
Now why would Big Oil ever agree to such a “Turn?” Well, the answer to that lies at your local Mickey-D’s. Yes, McDonald’s. You might have heard this story, but it’s a great one worth re-telling. Ray Kroc’s hamburger business was going poorly, and he was taking out personal loans to keep it afloat. A lawyer he brought in to review the business and give advice told Kroc his problem was simple: “you don’t quite understand the real business you are in. You are not in the business of selling burgers. You are in the business of real estate.” Kroc accepted this re-framing of his business proposition and made McDonald’s (with its standard menus and ingredients, franchises and leases) into the behemoth you behold today.
Big Oil realized more than decade ago that they weren’t in the gas business. They were in the energy delivery business. Oil and gas just happened to be the preferred energy products at a place and time, but what Big Oil was good at was delivering energy where and when it needed to be. The green energy advocates think they know the answer: electric cars and charging panels and charging stations. That is one possibility. Big Oil has run the scenarios, and they have made many small bets: electric cars and charging stations and solar, but also natural gas, hydrogen power, and driver-less cars and rigs, touch-less energy transfer, batteries, wind and hydroelectric and tidal power generation, even carbon-capture technology which (if it worked) could extend the POL-ICE combination. See, Big Oil is not sure which will win, and they are placing many bets, waiting to see what’s next.
Which recalls the last Turn, from horsepower to the POL-ICE connection. Some very sage experts in those times pointed out that a man on a horse could ride into the vast countryside with great assurance that he could provision his mount, as the countryside was where the hay was grown. What would happen when all those “drivers” started driving all those “automobiles” out of the city? They would litter the roadsides, out-of-fuel monuments to folly. Except that didn’t happen. Businesses grew to fuel and service the cars, governments built new and more and better roads, and something new and different happened.
All of which is a long way of saying the one thing Big Oil is NOT going to do right now is start many new leases, wells, or pipelines. They have been warned there is not much long-term future in fossil fuels, and they are think they are well-positioned to survive and thrive as “the Turn” commences, once it is clear which way it is going.
So let’s review, shall we. The POL-ICE era is ending, but no one knows how soon. Some advocates believe they know best how it will transition; most businesses and governments are hedging their bets, as there is a fortune to be made or lost. Big Oil may be the least likable business consortium since Big Tobacco. The oil and gas business is (and has always been) cut-throat but very profitable if you can stay ahead of the market. The major inputs to the retail price of gasoline are the price of a barrel of crude oil, taxes, station operating expenses and profit, in that order (from greatest to least). The only way to affect immediate supply and demand in the gas and oil business is to either shut down production or delivery (see the Arab Oil embargo in 1973) or to drastically decrease consumption (see the recent Covid economic collapse). There is no way to quickly increase the supply, unless there is untapped potential being intentionally withheld from the market. The only case where that currently applies is Saudi Arabia, who can literally turn on the spigots, but they are not in any way disposed to do so, nor have they (apparently) been given an impetus or inducement to do so. Saudi did just agree to increase production in the five year time-frame. Higher prices at the pump lag behind reductions in oil prices because that is how the industry (from Saudi Aramco to Bill at the corner station) keeps profitable.
You will see Congressional hearings soon, and both Republicans and Democrats will trot out the same hackneyed talking points we disabused here. Don’t fall for it; don’t re-tweet them or like their social media posts. Gas prices are high for very obvious reasons. You don’t have to like it (I don’t), but be smart about the subject, not partisan. And for God’s sake don’t drive the speed limit in the passing lane.
When we lived in the DC metro area (now called the DMV, for reasons I will never fathom, but this is the same place after all that named its football team the “Commanders”), it was common to not visit the famous memorial sites. One might drive by the monuments, but fight the traffic to find a parking place and visit them? Of course not, that’s for the tourists.
We live just 48 kilometers (30 miles) south of Guadalajara, Mexico’s second largest city, and we drive up every Sunday to a parish that hosts an English-language Mass. At various times we go shopping, or plan a night out to a fancy restaurant (with a driver and van back-and-forth). But this week we decided to stay a few days and check out our nearest big city.
It has its own song, dontchaknow?
Jalisco is Mexico, as the tourist slogan goes. And Guadalajara is the Capital of Jalisco, home to mariachi music, tequila, and the famous (all-Mexican) Club Deportivo de Guadalajara, aka Chivas! Most tourists know the cosmopolitan mega Ciudad de Mexico, or the various Atlantic or Pacific tourist resorts. But Guadalajara has much to offer, too, with less cost, fewer crowds, and much friendliness.
Guadalajara was founded in 1542, and gradually grew to incorporate many small towns which surrounded it: Zapopan (za-POE-pan), Tlaquepaque (tuh-LOCK-ee-pock-ee), Tonala (toe-na-LA). The city itself has a population of 1.5 million, but the Zona Metropolitano Guadalajara (ZMG) has over 5 million.
The sign times two, just like the songThe Teatro DegolladoLions, city symbolThe Founders Memorial
On Sunday we visited a few major religious sites and then wandered about the Centro area. Jalisco fashions itself the Catholic soul of Mexico, and it is home to several distinct shrines. First and foremost is the Guadalajara Cathedral, built in 1618 in a Spanish Renaissance style with two Gothic spires whose outline is synonymous with the city.
Anything look odd? Look closely!No, you weren’t imagining that: it is a horse’s head!
A second site of immense regional importance is the Basilica de Nuestra Senora de Zapopan, completed in 1689 in the Spanish colonial baroque style. This church houses a small doll of the Virgin Mary which was made by indigenous peoples in the seventeenth century and later became famous for several miracles: inducing peace among warring groups, ending plagues, and protecting from natural disasters. The figure visits the surrounding towns of Jalisco and is welcomed with parades, fiestas, and great fanfare. Her annual movement –called the Romeria–from the Cathedral back to the Basilica is a major municipal event. Over two million people join in the eight kilometer procession every October 12th. The Romeria is even recognized as a world cultural artifact by UNESCO.
The Virgin, andher Basilica
The final site is unfinished: the great Santuario de los Martires, which sits upon a high hill just south of the city center. This Church commemorates the twenty-five priests and laypeople martyred during the Cristero war, 1926-29. The design is futuristic, sometimes compared to a giant band shell. It is massive, and commands an amazing view of the city.
From the outsideGuadalajara skyline in the distancethe huge altar windowthe inside of the Church
We didn’t eat at any of the fancy (although inexpensive) restaurants this trip, but we did hit favorites like La Chata. Among our delicious plates:
FlautasFajitasChurrosOmelet with bacon and tomatillo saucePoached egg on English muffin with rich tomato sauceCrepas Tequila
Guadalajara has a full range of shopping opportunities. There are several high-end/fashion malls, but we don’t even visit such when we go to the States, so no we didn’t go there this time. Both Tlaquepaque and Tonala have excellent market areas with both artisanal shops and tourist junk: you have to be your own discerning consumer to ensure you’re shopping the former, not the latter. This trip we made it back into San Juan de Dios, aka Mercado Libertad, the largest indoor market in Latin America. The sprawling, three story complex is intimidating, with little organization and another mix of real, knock-off, and junk. But it’s also fun. Here’s a tip: the ground floor is mostly fruits, vegetables, meats, and flowers. The middle level is the grandest food court you’ve ever seen! The top level has stalls for everything else, from clothes to shoes to jerseys to electronics to leather goods to you-name-it!
A portion of San Juan de DiosTlaquepaqueTonala
We missed out on some of the cultural sites we wanted to visit, like the Palacio Gobierno (with its murals) and the State regional museum. Both were supposed to be open, but remained closed, possibly due to International Women’s Day (although we don’t know for sure). In the past this event has included protests and vandalism of memorials and buildings. We did witness the defacing of the Rotunda of Jalisco’s Illustrious Persons by these marchers.
Museo Regional de Jalisco, locked up tight.
It was a great trip and we only scratched the surface. Among other things we plan to do in the future: a Chivas match, Lucha Libre, and a visit to La Barranca de Huentitán (canyon). We’ve already visited the zoo, which is excellent (and well-shaded), and it also has views of the canyon.
One of the more famous Mexican renditions of the song Guadalajara was by Vincente Fernández, who just passed away last December. If you didn’t play the first version I provided, play this one, and get two Mexican classics in one!
Healthcare is probably concern number one to most expats; here’s the rather mundane story of out latest healthcare experience.
Judy started experiencing knee pain recently: actually, pain in the back of her knee, what we called her “knee-pit.” It seemed to be aggravated by exercise (how convenient!) or a lot of walking, so she cut back on those, did intermittent ice and heat, elevated it, and took over-the-counter (OTC) pain relievers for swelling and pain relief. Sometimes these standard remedies worked, other times they didn’t. Judy did the smart thing: she set a date certain, indicating if the symptoms didn’t go away by then, she was going to contact our doctora. During our recent mini-vacation in Manzanillo, we tried walking back-and-forth in the pool, the kind of low impact activity which should have helped; it didn’t.
So Judy contacted our primary care physician on WhatsApp. It’s a messaging app very popular around the world, except in the US. Individuals, businesses, even doctors give you their WhatApp number, which is just their cell phone number, and you can contact them directly to message or chat. It’s free and very convenient. Our doctora responded quickly that there was no need to come see her; she arranged us an appointment with a local specialist (again on WhatsApp) and we could go straight to see the orthopedista. Cost? Nada.
The orthopedista began the session by asking whether we preferred ingles or español; given this was a medical issue, we decided to stay with our mother tongue to be both clear and understood. He flawlessly changed to English and completed a brief history, then did a physical examination. He quickly identified where and when the pain happened in Judy’s knee; her sudden scream when he slightly twisted it was a dead giveaway! He told us the symptoms were indicative of a meniscus tear, which often will only be fixed by laparoscopic surgery, but the location was odd: it’s not where meniscus should tear. So he ordered up an MRI for further review. Cost for the consult: $1040 MXP or $50 USD.
Wait, wait, I know this one! It’s a knee!
Off we went to the MRI clinic (cost $6000 MXP or $300 USD) and got the results back (in Mexico in many cases, patients retain their own medical records, not the doctor or hospital, although a copy was sent to the orthopedista). The MRI technician gave us a large portfolio with a one written page of results, several panels of still shots from the MRI, and a disk with all the rest of the MRI shots on it. The written results indicated normal meniscus wear-n-tear, but also added there was a jug-handle tear (which would almost automatically indicate laparoscopic surgery). We could read and understand the Spanish diagnosis, but of course the MRI pics meant nothing to us. So we went back to our orthpedista with the results, expecting to schedule surgery.
Our orthopedista looked puzzled, read the text, then pulled out the pictures. He said there is no tear in the images, despite the text. He then loaded the disc up on his computer to investigate further. We waited, and then he resumed explaining to us that nowhere in any of the images is a jug-handle tear, so he wouldn’t know what to cut if he scheduled surgery, nor did he know why the written results did not agree with the images. He examined Judy’s knee again (very carefully this time, to avoid a repeat yodeling contest). He told me the fact that the back of her knee hurt, and only at a point in rotation, and more so with twisting, was “weird.” I concurred. Cost for this consult: $1000 MXP or $50 USD.
He prescribed an anti-inflammatory and scheduled an ultrasound in Guadalajara with a specialist he knew well and trusted. While an MRI is great for looking at harder objects (think bones), ultrasound ignores them and shows softer tissue (like ligaments and tendons). The orthopedista said this would be a final check on the issue of a meniscus tear, while clarifying if ligaments or tendons were involved.
So we tramped up to Guad for an ultrasound (cost: $1500 MXP or $75 USD). During the exam, the specialist told us (in English, which he apologized for in perfect accent and vocabulary) that Judy’s knee meniscus was fine. He spent some time looking at the back of her knee via the ultrasound, and concluded she had tendinitis in the popiletus, a tendon at the back which gives the knee stability. He sent the results to our orthopedista and we prepared for another consult.
Our final trip to the doctor was short and sweet. Judy’s course of prescription anti-inflammatory medication was working wonders: no pain for several days. The orthopedista told us he concurred with the specialist: tendinitis, requiring only more anti-inflammatory medicine, rest and recovery. Judy could start slowly to exercise in two weeks, and come back if the pain returned. (cost of consult: $520 MXP or $26 USD).
Total cost for an MRI, an ultrasound, and three visits to the orthopedista: $9540 MXP or $ 475 USD. We may never know why the first MRI specialist indicated a jug-handle tear, but the mistake was caught and fixed. We were quite pleased the orthopedista, who specializes in laparoscopic surgery, did not rush to cut, but rather kept saying he “would not cut unless he knew precisely what he would find there.” Overall, a positive experience at a very reasonable price.
You could be excused if you believed you had fallen asleep and awoke to find yourself in Europe in the 1930’s. Armies massing? Bogus staged provocations? Claims of the illegitimacy of neighboring states or governments? Interstate war? Same as it ever was.
“How did I get here?”
There is little surprising in Vladimir Putin’s invasion of Ukraine. Even recently, the Biden administration released unprecedented amounts of US intelligence clearly indicating Russia was preparing to do so, and US government officials made one dire prediction after another. These may have become background noise to some, but if so, those ignoring the warnings missed the true significance. Government officials rarely predict something as serious as war: they almost always emphasize first the ongoing negotiations and offer a tepid “war remains possible” walk off statement. In the past two weeks, US officials flipped the script: talking about how Russia was preparing, warning war was imminent, then giving a feeble “we still hope for negotiations.” It was a tell that an invasion was inevitable.
For some of us, this has been obvious for much longer. Long-time Russia hands remember seventeen years ago when Putin described the collapse of the Soviet Union as the greatest geopolitical catastrophe of the Twentieth Century. Neither the holocaust nor Nazism. Neither the holodomor nor the Khmer Rouge killing fields. Not Mao’s Cultural Revolution. The end of the largest authoritarian menace in history was what bothered Putin. Putin publicly dedicated himself then to re-establishing Russia as a great power, feared and respected by the world. Everything he did subsequently was toward that end.
Putin’s Russia will never be a world power, and he knows that. His economy is a mix of what we used to call Third World extraction (oil and minerals) and oligarchic capitalism, benefiting a few corrupt officials. Russian demography remains a disaster: rampant alcoholism and early male death, misogyny and violence leading to few marriages and even fewer births, a shrinking population unparalleled in peacetime. The average Russian is little better off than he was under Communism: and that is totally irrelevant. Putin has a iron grip on Russia itself: he openly jails political foes and kills dissidents with impunity. Russians either admire his strength or fear his vengeance. Remember, this is a country where you can stop in Red Square and take a tourist photo with a Stalin look-alike!
I guess Lenin got up and walked out of the tomb!
Long term, Russia remains in mortal danger, but Putin has played a mid-term game. Russia was initially too weak to do much but posture. He stabilized the Russian economy during oil price spikes and drops and solidified his position with the oligarchs: they know he will turn on them on a dime if they conspire against him, but they are free to make money if they don’t. He fundamentally remade the Russian military from a massive conscript force to a much smaller, more modern, volunteer force capable of threatening any neighbor, if not NATO writ large. He weathered the so-called color revolutions, losing a client state in Ukraine but holding on to Belarus. He threatened and invaded Georgia, putting its move toward NATO on ice. He has been welcomed into Kazakhstan, and has a “bond without limits” with China (no, I don’t believe this means much either, but it doesn’t hurt).
After President Obama failed to enforce his own red line in Syria (Assad’s chemical weapon attack), Putin moved quickly to ensure his Syrian ally’s security. Then he turned to Ukraine and unleashed his “little green men,” Russian Spetsnaz (special forces) which occupied ethnically Russian potions of the Donbas river basin and all of Crimea.
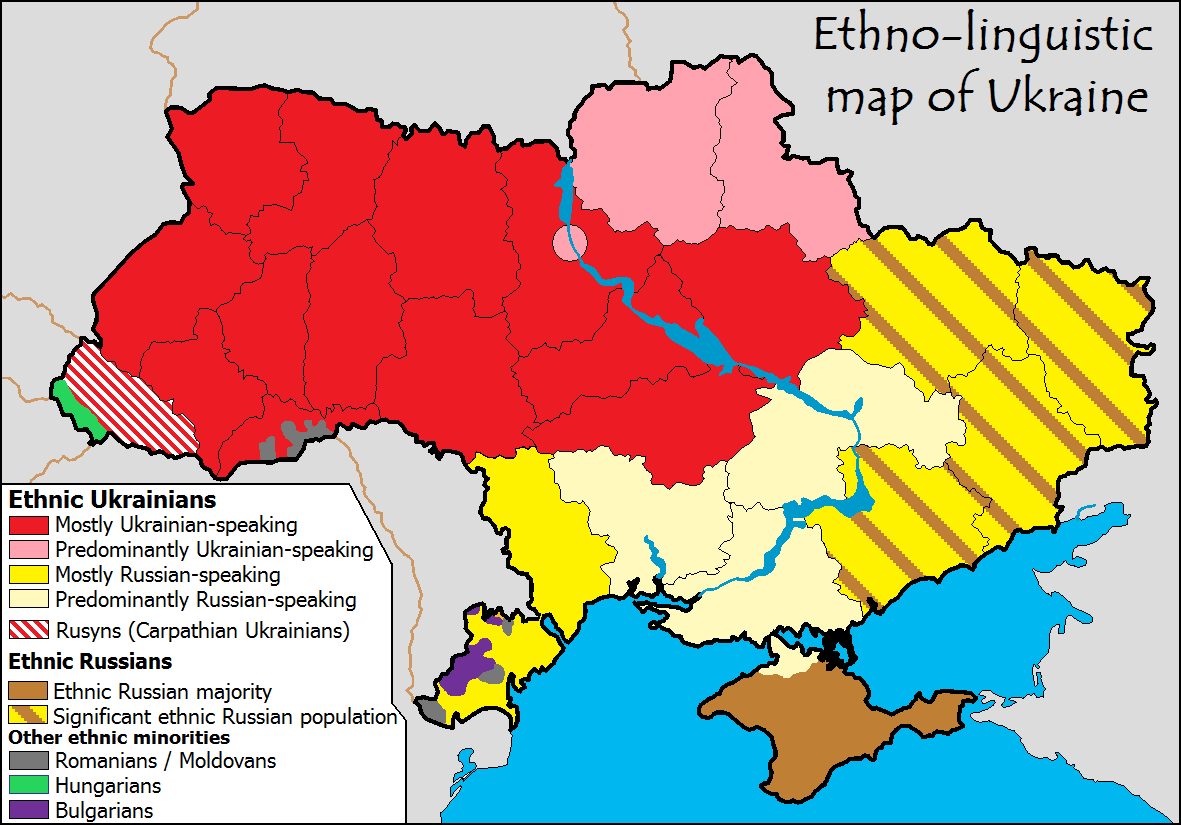
The blue line is the Dnieper river, a large and formidable obstacle. The pink circle on the river is Kyiv, the Capital.
Russia never accepted the Maidan revolution which had chased off a Russian-friendly government in Kyiv. The Crimea occupation was part practice and part toe-in-the-water experiment. Would the West respond forcefully to naked aggression covered with the only the most transparent fig-leaf? Sanctions indicated the answer was no, and the subsequent Minsk accords gave Russia some cover for its defacto seizures.
Meanwhile, Putin began preparing to finish the job. Russia amassed over $630 billion in hard currency (mostly non-US dollar) reserves in case of future sanctions. His oligarch friends probably did the same with their personal fortunes. The EU estimates current sanctions (pre-invasion) cost the Russian economy $50 billion annually. Assuming the new sanctions are twice as bad, Russia will run out of reserves in . . . only six and a half years! Putin negotiated agreements with friendly states, especially China, to continue trade without using dollars in the event of tightened US sanctions. He began a drumbeat in state-controlled Russian media to show Ukraine was a base of “NATO aggression” or “fascist forces” threatening ethnic Russians in Ukraine.
What happens now? Putin may stop at the Dnieper river to assess the situation. He may not try to take Kyiv in order to avoid the urban destruction and outrage that would entail. He may be willing to occupy ethnic Russian majority areas, establish a land bridge to Crimea and Moldova, and eliminate Ukraine’s access to the Black Sea. From these positions, Putin could pause to negotiate a cease fire and the establishment of a rump Ukrainian state with a government more amenable to Russia. He does not need to, nor does he probably want to, engage in a long-term occupation, which might become the focus of an insurgency.
The Biden administration was dealt a bad hand here: given Putin’s obvious intentions, the West needed to start to act long ago to deter him. However, every administration inherits bad situations, and they are responsible for resolving them. George W. Bush wanted to be “the education President,” focusing on America’s relations with Mexico and embracing “compassionate conservatism”: he got 9/11 instead. President Biden said he knew the world’s leaders on a first name basis; now has come his moment. The President has rightly rallied NATO, even encouraging Finland and Sweden to join in. But this won’t be over soon.
The administration said the array of increasing sanctions were designed to deter a Russian invasion: they have failed to do so. The EU and nations across the globe are joining in sanctions. But will they last? The NordStream 2 pipeline is completed; all Germany did was stop certification. In effect, some bureaucrat in Berlin took the pile of papers off his desk and put them in a drawer. They could resume certification in a moment. Europe needs Russian natural gas (Russia provides over 40% of Europe’s needs), and they cannot fully replace it with exports from the US. Oil prices have spiked to around $100 a barrel, which will further fuel inflation. Putin is betting he, his oligarchs, and the long-suffering Russian people can hold out longer than the–in his view–corrupt and irresolute West. He has a point. Most people forget that the very strict sanctions regime the entire world placed on Saddam Hussein was crumbling just before the Bush administration decided to go to war. We couldn’t keep sanctions on an insignificant country with a certifiable murderer-in-charge; can we do better with Russia?
Was Russian occupation of Ukraine inevitable? Putin took the measure of current Western leaders, and decided he could act. President Biden’s gaffe about a “small invasion” probably didn’t help, but what he said was true (NATO and the US weren’t going to fight to defend Ukraine), even though saying the quiet part out loud was the final nail in Ukraine’s coffin. Putin cannot afford war with NATO. While he would have tactical advantages in location initially, he cannot forestall a NATO build up and eventual counterattack. Any hint of ambiguity about US forces in Ukraine might have given Putin pause. For example, if Biden had rushed the US airborne forces not to Poland, but to Lviv (in far western Ukraine near the Polish border), to set up a permanent defensive perimeter for US diplomats, refugees, and perhaps the Ukrainian government, Putin might have occupied only the eastern parts of the country and steered clear. Even more so if Biden had convinced NATO allies to loin in the action.
Some will counter that American public opinion does not support going to war over Ukraine, and that is true. Neither do I. Yet American public opinion rarely supports going to war. Prior to provocation, the American public wanted to stay out of both World Wars. One major challenge of the presidency is to make the case for why the United States should go to war, if the President sees the need. President Biden ruled out making that case early on, following public opinion rather than leading it. One forgotten lesson of the Cold War is you can only deter an opponent if you have the capability and will to go to war with him; if the opponent doubts either your capability or will, he will not be deterred. The West can’t start the deterrence process by saying “we won’t fight under any circumstances.”
President Biden has announced tougher sanctions. A telling sign was the reaction of the US stock markets: while other markets around the world cratered on news of war in Europe, the US indexes rose! Why? They were expecting much tougher sanctions than the President imposed. We should assume Russia was warned: it makes no sense to rely on some sanctions with a threat of greater ones, if you don’t make it pretty clear how much worse it can get. In the meantime, there is much more the West can do, if the United States leads. All western airlines should be forbidden to land in Russia, and Aeroflot should be denied landing rights anywhere in the West. A review of all Russians on visas in the West for immediate expulsion, and a halt to all Russian visas in process. Russian consulates closed, Russian embassies reduced to minimum personnel. Of course no Russian athlete or team should be allowed into international competitions.
The US military could commence immediate production of ground-launched cruise missiles (GLCMs), once banned under the INF treaty (from which President Trump withdrew the US), and a replacement system for the Pershing II Intermediate Range Ballistic Missile. These two nuclear capable systems were the bane of Soviet leaders due to their short timelines (six minutes) to hit Moscow from Germany. The US should make clear to the Russian government that these weapons will be forward deployed in NATO countries IF Putin does not withdraw from Ukraine and re-establish the legitimate government in Kyiv.
The sanctions will hurt eventually, but will not soon force Putin’s hand. Instead, the West is in for a short (losing) contest for the future of Ukraine, but more importantly, a long contest to re-establish the notion of deterrence which has been lost. That means more spending on defense, more troops and agreements and exercises, more time and attention to foreign policy, and less time, attention, and money for everything else. All that just to maintain the status quo ante invasion.
Or Europe decides warm houses are more important than Ukraine. We lose focus. Americans resent double-digit inflation or a recession brought on by a massive rate increase by the Fed. China runs a sanctions evasion operation. And yes, China is watching how this all plays out for clues about its future interests in Taiwan.
For all intents and purposes, Putin has accomplished his initial objectives. Ukraine is his, and even NATO members like Latvia, Lithuania, and Estonia must be wondering about their security. Now the larger game is afoot. Does the US lead a reinvigorated NATO, and to what end? Do we find a way to pressure Putin and Russia to let go of Ukraine? Does China seize the moment, or simply lay low and provide Putin some cover? During the Cold War, every US presidential election had a subtext which went something like this: can this candidate stand up to the Soviet threat? Can they lead the free world, even if that means edging closer to war? That is a focus which was lost in the postwar period. Now it has returned with a vengeance.
On Valentine’s Day, 2065, the Department of Justice and the Food and Drug Administration dropped a bombshell: the US federal government had initiated criminal conspiracy charges against all major American sugar producers. Based on an enormous trove of evidence, sugar was the culprit for a wide-variety of health problems (obesity, heart disease, some cancers, autism and birth defects, even many mental illnesses). Furthermore, Big Sugar executives knew this as far back as the 1960’s, and engaged in a conspiracy to suppress the scientific data and even blame other products (remember the low-fat craze?). Millions of Americans, and other peoples worldwide, suffered and died due to the corporations’ actions.
Ever think you’d see a Mother Jones cover in my blog? Me neither!
Sugar immediately became the most suspect ingredient in history. The processed food industry began a race to the bottom of no-sugar in their products. Restaurants proudly posted signs proclaiming “we serve no sugar” or “take your sweet tooth elsewhere!” Sugar-free advertising became a badge of honor. But it didn’t stop there.
Of course, there was no Sugar Bowl college football game that year, or ever again. American sugar company stocks cratered, and advertisers turned down sugar sponsorship offers. The major media ran in-depth stories about the depth of the conspiracy: lies, pay-offs, political connections. Then media ran heart-wrenching stories of lives destroyed: everything from yo-yo dieters who had wasted their lives not realizing they were fighting a sugar addiction to families traumatized by children with autism or birth defects.
Predictably, the tone changed from the obvious (“Sugar is Evil”) to the more conspiratorial (“who knew what when?”). And there were plenty of targets. Big Sugar had many co-conspirators, from advertising agencies to scientists to politicians who played along. But it didn’t stop there.
Such a vast enterprise, operating openly for so long and causing so much heartache required a full and complete re-investigation of our history. Why didn’t federal bureaucrats stop this sooner? Why did some politicians not make this the top health priority? Why didn’t my doctor tell me? Where were the influencers, the sports heroes, the media personalities on this issue?
And so it began. The statue of former President Ron Desantis, who continued defending sugar long after it was obviously wrong, was defaced several times before being removed. Several high schools named for former first lady Michelle Obama dropped the association, since she was pro-nutrition but insufficiently anti-sugar. The House of Representatives changed the name of the Nancy Pelosi House Office Building to the Victims of Sugar Office Building, noting she never investigated Big Sugar while hoarding her designer ice cream. The University of Florida (America’s largest sugar-producing state) announced full-scholarships for students of families with disabilities associated with sugar use. The American Sugar refinery in Louisiana entered bankruptcy negotiations to settle claims for damages. Candy became a symbol of public disgust: you had to be a certain age to buy it in stores, and it was sold from behind the counter in unmarked paper bags. The NBA eliminated its LeBron James Award for Positive Corporate Relations after it became public he had invested in Big Sugar.
Alright, we’ve gone from the sublime to the absurd, so I think I have made my point. When you retroactively apply the thoughts, opinions, or even morality of today to the past, you must take care. I say this as a person who believes in moral absolutes; I always chuckle to myself when Progressives who say morality and truth are relative (to each person), then apply absolute tests of morality to historical figures. Not much for intellectual consistency, what? And to anyone out there thinking, “but Pat, you can’t be comparing sugar to slavery or Jim Crow or genocide or. . . “, I’m not. I am comparing the use of critical theory to history with a hypothetical future, to illuminate just how ridiculous it is, regardless of the seriousness of the subject matter. Plus, if you want to make the “slavery is far more serious argument”, okay, but what are you doing today given that there are almost twenty-five million people living in slavery now? Want to take responsibility for that? Or for ignoring it?
Much of what I wrote about sugar is true. It would not be surprising if some of the exaggerations I made later prove to be true, too. Sugar is terrible for you, it is addictive, Big Sugar did fight to blame fat for obesity and heart disease, politicians did and do protect sugar producers. And many if not most people know all this. Looking at our current lives with a “sugar-only” lens fails to consider how ubiquitous sugar is in our foods, how it causes cravings, and how many other MAJOR HEALTH CRISES compete for our attention. Life is more complicated today then where you stand on sugar.
One of the worst aspects of woke-ism is the assumption we moderns are morally and intellectually superior (because we are on the right side of history) and thus the application of today’s (superior) views to historical persons, places, or things. One might question the superiority of modern man (or woman). Where is today’s Lincoln or Washington? Da Vinci or Augustine? Mother Teresa or Jeanne d’Arc? We seem to have much more information at our fingertips, yet be much less well-informed. I see little reason to profess our intellectual or moral authority.
This is not an academic argument. The America represented in popular tracts like The 1619 Project is a practically-irredeemable place. As a young man growing up in a small town in Indiana, I was taught the standard fare of American history: the battles and the heroes and the missteps. I also learned about slavery, women soldiers in the Revolution and Civil War, the Japanese internment camps and the Jim Crow South. And I grew up far from any progressive educational paradise. All these things were covered in due course: briefly, and with context. If I had digested the American history put forward by Howard Zinn or the New York Times , I never would have dedicated almost forty years of my life to defending America and it’s constitution. Why defend the indefensible? Is that the goal?
G.K. Chesterton wrote in Orthodoxy, “Tradition means giving a vote to the most obscure of all classes, our ancestors. It is the democracy of the dead.” America, as a nation founded on an idea, has few common touchstones. You aren’t an American because of the way you look, or who you know, how you vote, how much money you have, or even how you got to America. You are an American if you believe in the idea of America. History is one of the few anchors our nation has. It must be history warts and all, as it happened and by its own standards at the time. Otherwise it is not history, it is an immature and unwise form of propaganda.
Subtitled “A Southerner’s Reckoning with the Myth of the Lost Cause,” this work is by Ty Seidule, Brigadier General (retired), and the first Professor Emeritus of History at the United States Military Academy. Seidule had his “fifteen minutes of fame” back in 2015, when he gave a talk for PraegerU, a conservative online site which produces short videos. Entitled “Was the Civil War about Slavery?” it became the most watched history video . . . in history.
Well worth five minutes of your time!
Spoiler alert: Yes, the Civil War was all about slavery. Seidule was shocked at both the popularity and the notoriety of this short video, which he thought rather obvious.
Seidule’s book builds on that experience to address the Lost Cause mythology of the American South. However, don’t expect a history book in the classic sense, or even a data-driven argument. Seidule adopted the personal-story-as-explanatory-history approach, very popular among authors today. Seidule’s personal history is as a young man who grew up in Alexandria, Virginia (a close-in suburb of Washington, DC, so close it was originally included in the District), a quintessentially southern town in the 1970’s.
In prose both fluid and florid, Seidule tells of growing up a privileged son on the south, taught to revere that ultimate southern gentleman, Robert E. Lee. During his youth, Virginia state history books still had outrageous depictions of plantation life complete with happy slaves and kindly masters! Alexandria especially tried to proclaim its Confederate heritage: the town was occupied on the first day–and for the duration of–the Civil War, so it literally named all its north-south streets after Confederate heroes.
BG(ret) Seidule notes he swallowed all these myths (State’s rights, contented slaves, chivalrous Confederates personally opposed to slavery but unwilling to end it) and fully believed them. Only as an adult and budding historian did he come to realize what a slanted version of history he had been fed, and he has dedicated himself to setting the record straight.
It should go without saying, but Seidule is absolutely right. The Civil War was about slavery. Slavery is uniquely horrendous at all times, and the behavior of post Reconstruction southern leaders in their successful attempts to rewrite history and enforce Jim Crow laws was egregious. Seidule is at his best uncovering the history he never learned about towns he lived in, like Alexandria and Monroe (Georgia), which was once known as “lynchtown.” He is at his weakest when he makes post hoc arguments about why things are without any footnote or reference. Here his book comes across with little force, more like an extended opinion piece in the New York Times magazine.
Further, Seidule relies on his righteous anger at being misled at key points. He does establish the fact that generations of southern children received similar brain-washing, which partially explains the staying power of the Lost Cause myth. But, he also recognizes most of this historical fiction ended by the 1980’s, so what we have now is . . . what? Street names? Statues? Today’s students in Northern Virginia (where I lived for thirty years) get barely a few hours of Civil War history, and are hard pressed to say anything intelligent about the war. Their ability to process the name of Lee highway or J.E.B Stuart high school as a public symbol of white supremacy is suspect.
Early in this work–in the Foreword, actually–Seidule relates the story of his involvement with a project to memorialize West Point alumni who died in combat. Seidule explains he opposed including those West Pointers who abandoned the country and the Constitution at the moment of greatest danger to join the Confederacy. He notes he was overruled by the Academic Board and even the Superintendent, before someone leaked the plan and public outrage led to his position (i.e., no Confederate names in the memorial) being adopted. So far, so good, and of course the Brigadier General was in the right.
But in the telling of the tale, Seidule says “I should have realized that the overwhelmingly [sic] white men around the table might have grown up with the same myths, really lies, about the Civil War.” He has no footnote, no evidence, just a bold-faced assertion of the private thoughts and beliefs of his follow officers. This is unfortunate.
How did he know? He never says. Was there not another possibility? As a professional historian, he knows there was. I attended West Point around the same time Seidule was at Washington & Lee. Cadets did indeed study Lee, the officers who abandoned the Union, and the issue of slavery in the Civil War. In Military Art classes, we examined in-depth Lee’s tactical and operational brilliance, and his manifest failings as a strategist. In ethics, while we examined the role of States in the early days of the Republic and the loyalties they entailed, we also firmly established that abandoning our oath in wartime was an act of treason. Some cadets found this hard to swallow, but I never heard anything else than that from the faculty.
Finally, in studying how wars end, we learned about the unique outcome of the American Civil War. Most such conflicts end only with reprisals, widespread destruction, and endemic hostility. The US Civil War was different: it ended with the successful re-integration of the seceding states. This was in no small part due to the guidance of President Lincoln, whose wartime Second Inaugural address said “with malice toward none except the damn rebels, with charity toward all except the racist traitors.” You know the italicized words ring false because they weren’t there. Lincoln told Congress his plans to pardon the Confederate soldiers upon conclusion of the war. President Andrew Johnson issued a conditional pardon shortly after the war, and he followed that up with an unconditional pardon on Christmas day, 1868. Thus began the process of re-integration of the Union, which was uniquely successful.
Seidule confuses this part of the historical record with the shameful failure of Reconstruction, the abandonment of the freedmen, the introduction of Jim Crow and the racism in both north and south that continued to the Civil Rights era. These things did follow, but they were not necessarily caused by the pardoning process, which worked. He suggests any reference (picture, naming, statue, etc,) to Lee is part and parcel of the Lost Cause mythology and therefor suspect. Seidule rightly holds dear to the US Constitution and the oath that he and I took to defend it against all enemies, foreign and domestic. Yet that pardoning power is part of that same Constitution, and he rejects it. Here his anger at being misled gets the better of his argument.
Robert E. Lee was a great leader and a fine military officer. He was also a racist who personally benefited from, and directed the mistreatment of, slaves. He was at once refined AND cruel, educated AND ignorant, kind AND intolerant. The author is right to decry the fact he was led to believe only one side of history. Would that he had heeded that advice here.
My verdict: if you were led to believe only in the ‘sainthood’ of Robert E. Lee, this work is a powerful corrective. If you were ever exposed to the more complicated story of Lee and the South, you’ll find much of this book unsurprising.
We decided to take short trip (this week) out of lakeside to see the Pacific Ocean, and we chose the port of Manzanillo (Mahn-zah-NYEE-oh) in the state of Colima. Mexico’s Pacific coast is full of promising locations to visit, from Los Cabos on the tip of the Baja Peninsula to Mazatlan, Puerto Vallarta, Manzanillo, and finally Acapulco. While Acapulco was the first of these to breakthrough as a tourist destination in the 1940s, Puerto Vallarta is undoubtedly the most popular today. Why Manzanillo? Why not?
The bay from our balcony
What makes Manzanillo different from the other tourist destinations mentioned above is its status as Mexico’s largest port, and the main hub for Mexican trade across the Pacific. This gives the town a working-class patina that probably would never let it turn into a full-scale tourist town. Still, it does have a fair number of tourists, especially Canadians and Mexicans (we arrived on Constitution Day, a federal holiday in Mexico, and many Mexican families were ending a long weekend visit at the condominio where we stayed).
Port in the distancefreighters waiting to dock
What’s the draw? It is easy to reach from Guadalajara, with only a four hour drive from lakeside (assuming I’m driving! “Your mileage may vary” as they say.). The weather is beach classic: averaging around eighty-five degrees Fahrenheit in February, with lows in the mid-sixties. It is much less crowded: no cruise ship stops, and fewer direct flights from the States (four) or Canada (only one), and more than a days drive from the border. For these reasons, Manzanillo is far less expensive than other Pacific resorts, especially PuertoVallarta. Both have restaurants, resorts, hotels, and attractions across the price range, but generally they will be less expensive in Manzanillo.
We’re not big on water sports, but Manzanillo is. It fancies itself as the sail-fishing capital of the world, and holds an annual contest to back up the claim. There’s a near-shore shipwreck for scuba and snorkel fans, plenty of public beaches (all are in Mexico), and fishing and whale-watching boat charters galore, with options to drink enough to see whales whether they’re there or not!
As one would expect, the food in general–and the seafood in particular, has been very good:
Caprese salad and musselsCarbonara and Mahi-mahi
Two large appetizers, two full main plates, two glasses of wine ran us under $50 USD (beats Red Lobster, no?). We regularly drove out of our condominio and visited places along the main drag in town and found it easy to navigate and perfectly safe. We especially liked a small local restaurant called Juanitos, which was packed with locals for breakfast.
One final note. If you’re like me, you might have confused Manzanillo with La Manzanilla (both are named for the Manzanilla tree, used by Spanish explorers in Mexico to build ships to cross the Pacific as early as 1522!). La Manzanilla is a much smaller fishing village north of Manzanillo. If you’re trying to get totally away from the tourist vibe, you’ll want to try La Manzanilla. Both are worth a visit, based on what friends have told me.
Final verdict: Manzanillo is budget-friendly, easy to reach (for expats), with great beach weather and ample beaches, and excellent water sports. I would recommend it for those who find large tourist destinations too crowded or expensive, but who still seek the classic Mexican beach vacation on the Pacific side.
Something about the date today got me thinking, and I suddenly realized we’re approaching our fifth anniversary (February 1st, 2017) of moving to Mexico. Tempus fugit and all that. Which got me to thinking about what has changed, what hasn’t, what’s new, what isn’t and all other things expat.
The climate remains spectacular. I’m sitting on my terraza looking out at the lake at 9:00 in the morning in late January, wearing shorts and a t-shirt. The sky is blue, with just a few puffy clouds, and the temperature will hit seventy degrees Fahrenheit shortly; next week we’ll reach eighty. All this with no threat of hurricanes, tornadoes, tsunamis, earthquakes . . . wait, we do have an active volcano, but it’s far away and not that active, I think. Anyway, the climate is still as good as advertised. Some expats claim it is getting colder in winter (due to climate change) but the weather data has changed little. I know that these five years have weathered me to the point I no longer handle cold well. I used to run in the snow in a t-shirt and shorts; now fifty degrees gives me the chills.
The Mexican people are as friendly and welcoming as ever. One would think the pandemic might have put a dent in their good humor, but they choose to look at it all as just another part of life. No carping about difficulties in getting vaccines or masks. No complaining about restrictions, except in that like all government rules, they may be more honored in the breach. Few people getting all exercised about other people’s pandemic behavior, with the exception of a television announcer in Guadalajara:
Turns out he’s more of a performer than a newscaster!
In general, life continues apace here in Mexico. The government never (really) closed the borders, only shut things down for a week here or there, and mandated some performative measures. Some stores or restaurants still have a wet rag on the floor at the entrance, to “sterilize” your shoes before entering, from back when health officials thought Covid was a contact threat. You step on it, then on a dry rag next to it, pump some anti-bacterial gel onto your hands and enter. Sometimes someone waves a magic thermometer at you: they keep trying until they get a result allowing you to enter. Go figure: the results in illness, hospitalization, and death rates are about the same here as in the States, just without all the drama.
It is still cheap to live here, although housing and rental prices have become challenging to some. Mexico’s inflation rate was over seven percent last year, but the peso exchange rate has varied between twenty and twenty-two pesos per dollar, effectively negating the inflationary effect on expats. The rising cost of living is reflected in a rising federal minimum wage ($173 MXP, or about eight dollars a day), which in turn raises the amount needed for an expat to qualify as a temporary or permanent resident. Likewise, Mexico is tightening its immigration enforcement, meaning we’ll see fewer digital nomads (younger folks working online), fewer boomers retiring to Mexico to live on just Social Security, and fewer free spirits who just come with a backpack and overstay their tourist visas.
What about the current expat composition? Snowbird numbers were down during the pandemic, even though the airline routes remained available. The sizable population of Canadian snowbirds (loons?) suffered some pretty strict federal rules that severely limited their ability to visit. Ottawa used everything from threatening to eliminate access to health care to mandatory, supervised, and expensive quarantines to reduce the number of Canadians travelling abroad. American snowbirds numbers were somewhat reduced due to fear of getting severely ill in another country, but are beginning to rebound. Why? During an average year, about one million baby boomers retire (those numbers usually declined during recessions); during this pandemic, the number of baby boomers retiring has more than tripled and appears to be accelerating! All of them have to go somewhere.
Those in the States already know about the nation-wide escalation in home prices, and it’s especially fierce in warmer, nicer places to retire. We have seen a small increase in housing costs here, but much more of an active market, as the wave of baby boomers look south at the same time the newly-retiring Mexican middle class catches on to the notion of a leisurely retirement in a great location (rather than staying put in the family home).
And these trends prove out in the anecdotes we hear, and our own experiences. While construction has slowed during the pandemic, many new projects are suddenly springing up or back-to-life. Our web boards and social media are filled with potential expats asking the usual questions, planning a reconnaissance trip, or announcing they’re in town and looking to make new friends. Some of the long-term expats we arrived with (or shortly behind) are looking to return to the States, for all the usual reasons: increasing health concerns, separation from family, or death of a spouse. There is a constant churn among the expat community for these reasons, none of which reflect on any expat’s rejection of lakeside, but simply a change in life circumstances necessitating a change in domicile. Speaking of change of domicile, we moved late last year, and I will soon have a little tour of our new place in another post.
What’s the verdict, five years in? Of course we still love it here, or else we wouldn’t have gone all-in in buying a new house. All the things we loved about the town and the country continued; we have added a few new ones. We never anticipated being expats in the midst of a pandemic, but I would argue it has been easier here than anywhere else. Mexico presents no challenges to our ability to travel the world or to return to the States as often as we like: no requirements whatsoever from this end. We ended up being the only members of our immediate family able and willing to travel, so we went to see everyone else as they hunkered down: South Bend, Cincinnati, Baltimore, Wolfeboro (NH). Whenever a country decided it could safely allow tourists, we jumped on the bandwagon: Greece in June, Italy in November. We will continue the torrid pace this year, with a French river cruise plus land tour in May, Thanksgiving in Italy with a side tour to Sicily, and another round of visits to family. All this is made possible by the low cost of living and the ease of travel. And as Mexico seems to be moving to treat Covid as an endemic disease, we plan to take more local trips to places like Manzanillo, Guanajuato, and Oaxaca.
While the increasing number of expats locally do clog up the relatively small number of streets in our little town, I can’t get angry about it. Being an expat is not for everyone, but for those who relish a little spice in life, it is wonderful. I can’t bring myself to get angry about folks who are just trying to discover (like we did) whether the expat life is right for them!































![Robert E. Lee and Me: A Southerner's Reckoning with the Myth of the Lost Cause by [Ty Seidule]](https://m.media-amazon.com/images/I/51YuVl5A1TL.jpg)




